Pathogenesis
Gastrointestinal (GI) cancers, including gastroesophageal adenocarcinoma and biliary tract cancers are a part of a heterogenous group of malignancies with HER2 status as an important feature.1 HER2 amplifications and/or overexpression are associated with distinct clinical and pathological features in GI tumors and associated with a worse overall prognosis.2
Gastroesophageal adenocarcinoma (GEA)
GEA, arising from the stomach, gastroesophageal junction, or distal esophagus, is usually diagnosed at an advanced stage, resulting in poor prognosis.3,4 This may be potentially related to diagnosis as advanced GEA (defined as unresectable local-regional, recurrent, or metastatic disease).4,5 Despite treatment with systemic chemotherapy, median overall survival with advanced or metastatic disease is 10-12 months.4 Moreover, high relapse rates have been observed after curative surgery for non-metastatic tumors.4
The most frequent histologic variant of gastric adenocarcinoma is the “intestinal type”, with a model of pathogenesis of progression from chronic gastritis, inducing chronic inflammation, metaplasia, dysplasia, and eventually adenocarcinoma.6 Similarly, ~60% of distal esophageal and GEJ adenocarcinomas arise from Barrett’s esophagus metaplastic epithelium.6
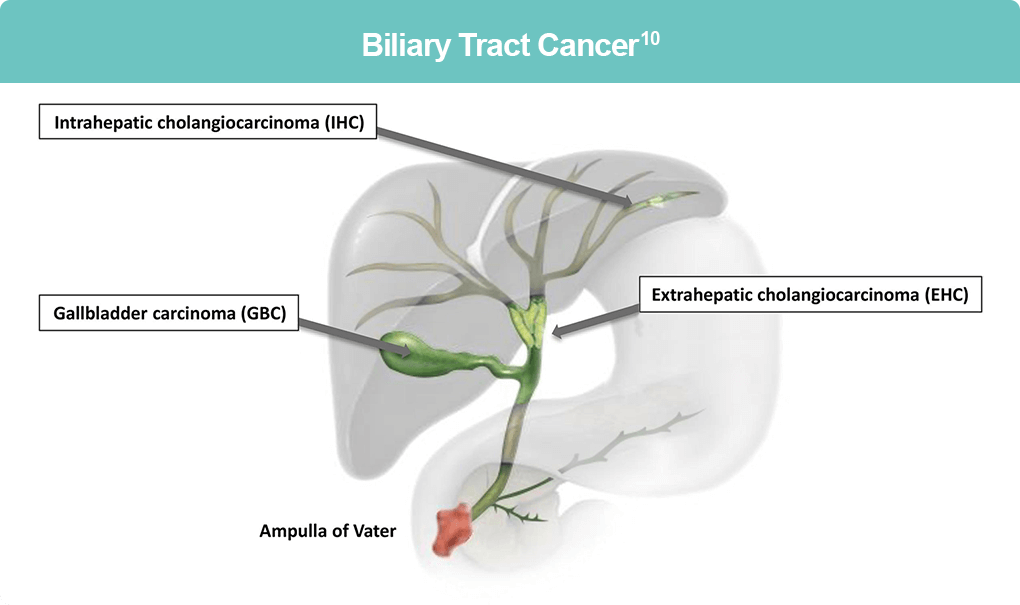
Biliary Tract Cancer (BTC)
BTCs are a rare and aggressive group of cancers, including intrahepatic cholangiocarcinoma (CCA), extrahepatic CCA, gallbladder cancer, and ampulla of Vater cancers. Gallbladder cancer is the most common BTC, of which the majority are adenocarcinomas; characteristics include shorter medial survival, shorter time to recurrence and shorter survival after recurrence than hilar CCA.7 Gallbladder tumors located on the hepatic side have a worse prognosis, although identification of the original tumor location may be difficult due to tumor spread.7 Most CCAs are adenocarcinomas (>90%), with extrahepatic CCAs being more common, however, intrahepatic CCAs often have a late presentation. 7 BTCs represent about 3% of GI cancers and have only a 2% 5-year survival rate; in fact, less than 35% of BTCs present with resectable disease.8,9
The pathogenesis of BTC is mediated through an inflammatory state that is induced by the release of pro-inflammatory mediators, such as interleukin-6, tumor necrosis factor-a, cyclooxygenase-3, and Wnt. The resulting damage leads to aberrant bile acid signaling and activation of growth factors that promote cholangiocyte proliferation. These changes promote the accumulation of genetic and epigenetic alterations in tumor suppressor genes, proto-oncogenes, and DNA mismatch repair genes, leading to activation of ERK1/2 and NF-κB pathways that encourage uncontrolled cell growth, survival, angiogenesis, invasion, and metastasis.11,12
Molecular drivers of GEA and BTC
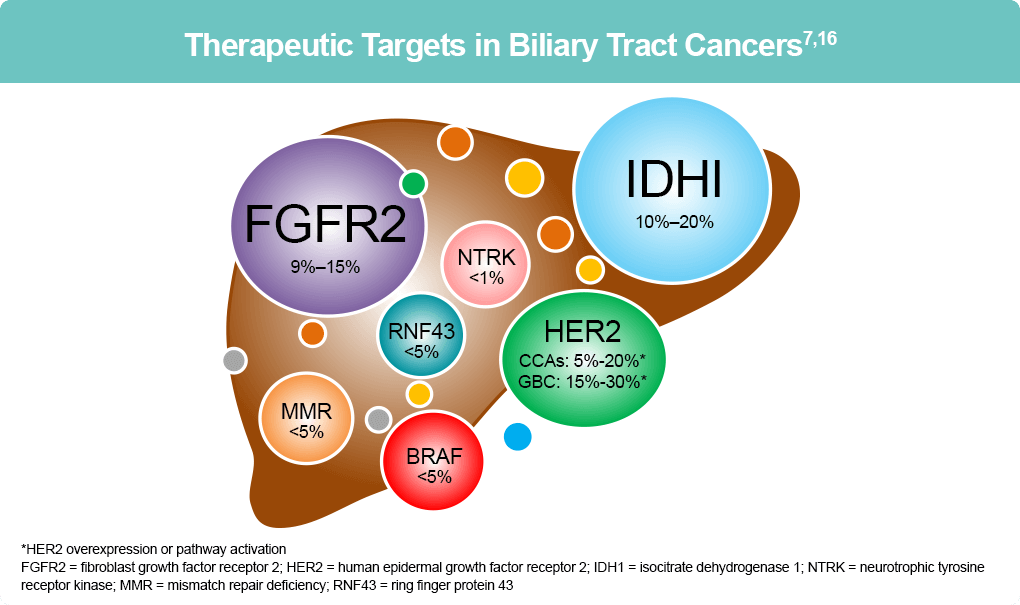
GEAs and BTCs can be driven by various molecular mechanisms, which may be useful as therapeutic targets.4,10 HER2 (also known as ERBB2) is a proto-oncogene located on chromosome 17q21 that encodes a tyrosine kinase receptor, a member of the epidermal growth factor receptor (EGFR) family.13 Remarkably, between 7%-38% of GEAs demonstrate HER2 amplification and/or overexpression, while in BTC, 5%-15% demonstrate HER2 amplifications, 20% HER2 overexpression, and 2% HER2 mutations.8
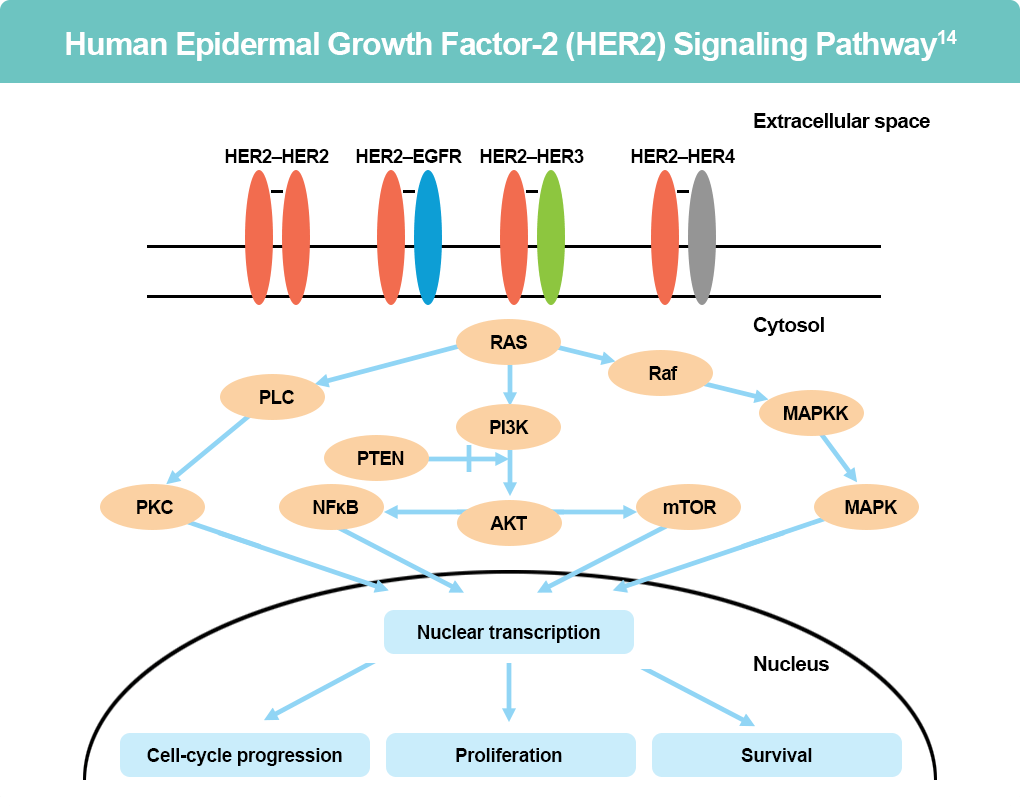
HER2 lacks a known exogenous ligand and is activated by its interaction with other HER family members and other tyrosine kinase receptors. Phosphorylation of HER2 initiates various signaling pathways that are responsible for cell division, proliferation, differentiation, and anti-apoptosis signaling, converging in two fundamental pathways: the RAS-MAPK (mitogen activated protein kinase) pathway and the PI3K-AKT pathway.3,15 HER2 is the first receptor targeted successfully in GEA, with trastuzumab being the first unique target agent that was FDA-approved as the standard of care (SOC) in the first-line treatment of HER2 positive GEA.4
Additionally, there are several emerging molecular mechanisms that have been identified in GEA influencing carcinogenesis, such as activation of the RAS-RAF-MEK-ERK, PIK3CA-AKT-mTOR and JAK pathways with fibroblast growth factor receptor (FGFR), tumor angiogenesis with vascular endothelial growth factor receptors (VEGFR) and angiopoietin-2, and tight junctions with Claudin 18.2.4

Importantly, GEAs can demonstrate differing molecular profiles over time and can be influenced by treatment, indicating the importance of repeating tumor profiling with any evidence of progression.4 Understanding the changes in the tumor profile may be advantageous in tailoring treatment approaches to achieve precision care in second and later-line settings.4
There are also a number of emerging oncogenic molecular targets in BTC, including fibroblast growth factor receptor (FGFR2), fibroblast growth factor receptor 2 (FGFR2), and neurotrophic tyrosine receptor kinase (NRTK).16 Notably, genetic driver mutations can vary between differing CCA subtypes.16
References
- Kelly RJ, Bever K, Chao J, et al. Society for Immunotherapy of Cancer (SITC) clinical practice guideline on immunotherapy for the treatment of gastrointestinal cancer. J Immunother Cancer. 2023;11(6):e006658. doi: 10.1136/jitc-2022-006658
- Zheng-Lin B, Graham RP, Bekail-Saab TS. Targeting ERBB2/HER2 genetic alterations: An expanding therapeutic opportunity in gastrointestinal cancers. Chinese Clin Oncol. 2023;12:55. doi:10.21037/cco-23-72
- Bartley AN, Washington MK, Ventura CB, et al. HER2 Testing and Clinical Decision making in Gastroesophageal Adenocarcinoma: Guideline from the College of American Pathologists, American Society for Clinical Pathology, and American Society of Clinical Oncology. Arch Pathol Lab Med. 2016;140:1345-1363. doi:10.5858/arpa.2016-0331-CP
- Petrillo A, Smyth EC, van Laarhoven HWM. Emerging targets in gastroesophageal adenocarcinoma: What the future looks like. Ther Adv Med Oncol. 2023;15:17588359231173177. doi:10.1177/17588359231173177
- Li W, Zhang X, Du Y, Zhang Y, Lu J, et al. HER2-targeted advanced metastatic gastric/gastroesophageal junction adenocarcinoma: Treatment landscape and future perspectives. Biomark Res. 2022;10:71. doi:10.1186/s40364-022-00416-x
- Mukkamalla SKR, Recio-Boiles A, Babiker HM. Gastric cancer. Last updated July 4, 2023. StatPearls. https://www.ncbi.nlm.nih.gov/books/NBK459142/
- National Comprehensive Cancer Network®. NCCN Clinical Practice Guidelines in Oncology. Biliary Tract Cancers (Version 1.2025) https://www.nccn.org/professionals/physician_gls/pdf/btc.pdf
- Ayasun R, Ozer M, Sahin I. The role of HER2 status in biliary tract cancers. Cancers. 2023;15:2628. doi:10.3390/cancers15092628
- Kefas J, Bridgewater J, Vogel A, Stein A, Primrose J. Adjuvant therapy of biliary tract cancers. Ther Adv Med Oncol. 2023; doi:10.1177/17588359231163785
- Athauda A, Fong C, Lau DK, et al. Broadening the therapeutic horizon of advanced biliary tract cancer through molecular characterization. Cancer Treat Rev. 2020;86:101998. doi:10.1016/j.ctrv.2020.101998
- Marcano-Bonilla L, Mohamed EA, Mounajjed T, Roberts LR. Biliary tract cancers: epidemiology, molecular pathogenesis, and genetic risk associations. Chinese Clin Oncol. 2016;5: doi:10.21037/cco.2016.10.09
- Labib PL, Goodchild G, Pereira SP. Molecular pathogenesis of cholangiocarcinoma. BMC Cancer. 2019;19:185. doi:1186/s12885-019-5391-0
- Abrahao-Machado LF, Scapulatempo-Neto C. HER2 testing in gastric cancer: An update. World J Gastroenterol. 2016;22:4619-4625. doi:10.3748/wjg.v22.i19.4619
- Iqbal N, Iqbal N. Human epidermal growth factor receptor 2 (HER2) in cancers: Overexpression and therapeutic implications. Molec Biol Int. 2014;2014:852748. doi:1155/2014/852748
- Tirino G, Pompella L, Petrillo A, et al. What’s new in gastric cancer: the therapeutic implications of molecular classifications and future perspectives. Int J Mol Sci. 2018;19:2659. doi:10.3390/ijms19092659
- Personeni N, Lleo A, Pressaiani T, et al. Biliary tract cancers: Molecular heterogeneity and new treatment options. Cancers.2020;12:3370. doi:3390/cancers12113370
All URLs accessed April 12, 2025