What is GEA & BTC?
Gastroesophageal adenocarcinoma (GEA) and biliary tract cancer (BTC) are both cancers of the digestive system.1 They have several common features including overexpression of the human epidermal growth hormone receptor 2 gene or HER2 that is responsible for cell growth, poor prognosis when diagnosed at an advanced stage, and a tendency for heterogeneity, meaning differences in cancer cells within the same tumor.1
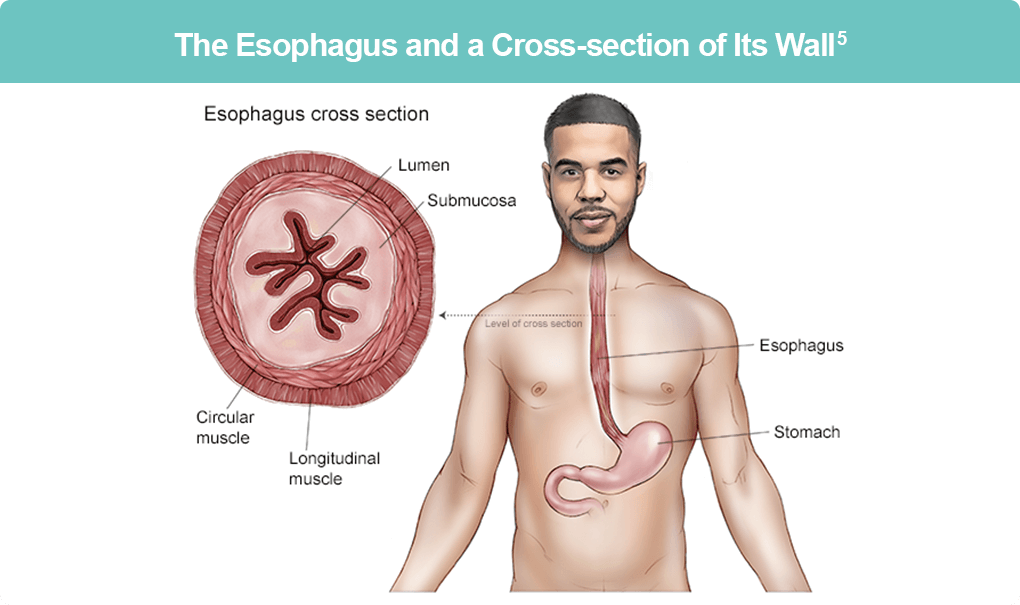
The esophagus is the tubular structure (approximately 10 inches long and an inch wide) connecting the throat to the stomach, and esophageal cancers typically start with abnormal cellular growth in this region.2 There are two types of esophageal cancers, GEA, which starts in the mucus-making cells of the esophagus and is found in the lower to mid-esophageal regions, and esophageal squamous cell carcinomas (ESCC) that start in the flat cells in the inner lining of the esophagus. Tumors that start in the stomach but extend into the esophagus (at the gastroesophageal junction, which is where the stomach and esophagus meet) are treated as GEA and are the more common type of esophageal cancers in the United States.2 These stomach, gastroesophageal junction, or distal esophagus cancers, when diagnosed at an advanced stage, have a poor prognosis.3,4
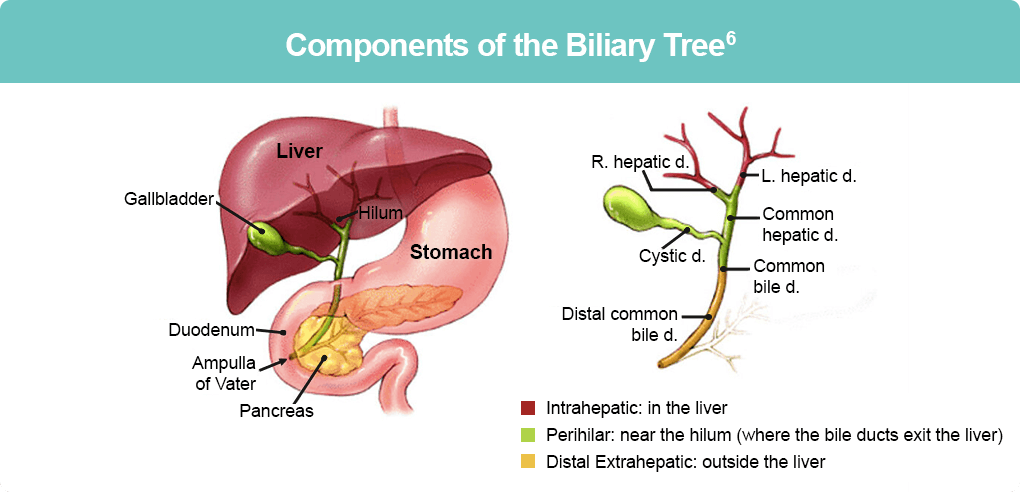
Hepatocytes or liver cells secrete bile into the intracellular spaces in the liver from where the bile drains into the left and right hepatic ducts (intra-hepatic bile ducts). From here the bile travels via the common hepatic and cystic ducts to the gallbladder. The cystic duct releases bile into the common bile duct (extra-hepatic bile duct) and from there into the small intestine (duodenum) to help digest fat in ingested food.6 BTCs or cholangiocarcinomas include cancers of the gallbladder, intra-hepatic and extra-hepatic bile ducts, and the ampulla of Vater (these are the ducts that connect the liver and pancreas with the small intestine).7
Diagnosis
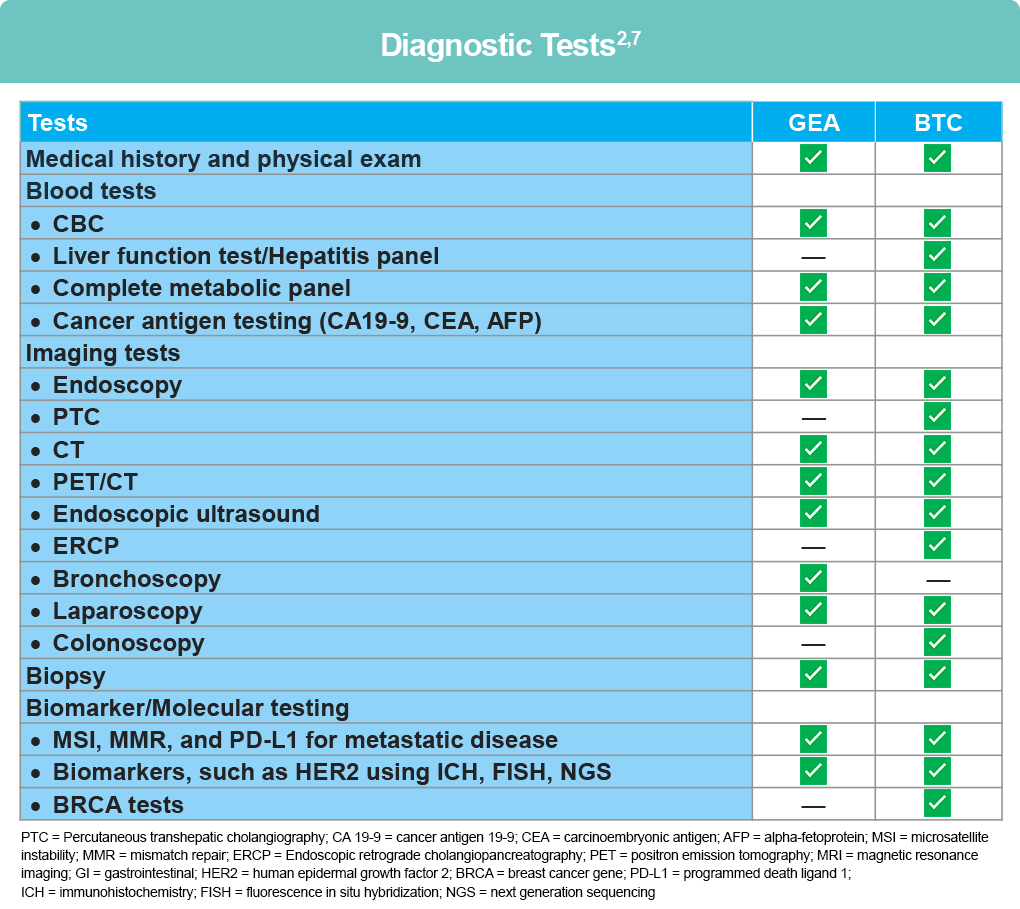
Patients with GEA and BTC are diagnosed depending on the type of cancer suspected, various signs and symptoms, age, general health of the patient, and results of any previous test results.5 Diagnosis of GEA and BTC is done based on medical and family history of the patient, a physician exam, and results from various blood tests, imaging tests, and biopsy. Additionally, in case of advanced GEA and BTC, testing for biomarker, such as HER2 will help to determine treatment options. A detailed explanation of tests that may be used for diagnosis of GEA or BTC can be found in the patient guidelines for esophageal cancers2 and gallbladder and biliary tract cancers.7
How are GEA and BTC Diagnosed?2,7
Blood tests, such as the complete blood count or CBC measure the levels of various blood cell types including red blood cells, white blood cells, and platelets providing vital information on your body’s ability to carry oxygen to various body parts, fight an infection, and aid in blood clotting. Other blood tests may include a comprehensive metabolic panel or CMP that relays information about kidney and liver functioning and a liver function panel that can relay information about the health of the liver.
Imaging tests, such as an endoscopy, CT scan, MRI scan, PET scan, or ultrasound are used to visualize the gastrointestinal tract. For example, an endoscopy is performed using an instrument called the endoscope that has a light and camera attached to it, and that is inserted down the throat, the esophagus, stomach, and upper parts of the small intestine while the patient is under sedation. Similarly, a percutaneous transhepatic cholangiography or PTC uses a contrast dye and an X-ray to take pictures of the biliary tract. A CT, MRI, or PET scan is typically used to learn the extent of cancer spread or staging of the cancer. Stages of esophageal cancer range from 0 to 4, and a staging of 4 is indicative of cancer that has spread beyond the esophagus to the lymph nodes and other parts of the body (ie, metastatic GEA).2,5 For BTC, the TNM scale is used, which measures Tumor location, lymph Node involvement, and Metastasis or spread to distant parts of the body. As with GEA, stages range from 0 to 4B, with 4B indicative of metastatic BTC.7
A biopsy is performed if an abnormal region is detected during an imaging exam. This involves removing a tiny amount of fluid or tissue from the suspicious area, followed by a pathological examination of the tissue. This can be used to help make a definite diagnosis of the cancer. Examples of biopsies include a fine-needle aspiration and a core needle biopsy depending on the type of needle used to extract tissue.
Biomarker or Molecular testing/Tumor profiling uses a biopsied sample to look for specific gene mutations/alterations, protein levels, and other molecules that may be unique to the tumor and aid in treatment decision-making.2 An example of a protein that is commonly overexpressed or amplified in cases of GEA and BTC is HER2 or human epidermal growth factor receptor 2. Drugs that target HER2 can be used to treat HER2 ‘positive’ patients as these drugs will only be effective in patients with too much of HER2 protein.2,7
Diagnosis of differing subtypes of BTC can be challenging. For instance, with gallbladder cancer (GBC), diagnosis is often incidental at cholecystectomy and typically of advanced stage, due to lack of symptoms or symptoms that mimic biliary colic/chronic cholecystitis. Guideline recommendations for initial workup of GBC includes liver function testing, computed tomography (CT) and/or magnetic resonance imaging (MRI) of the chest, abdomen, and pelvis for assessment of tumor penetration through the gallbladder wall as well as nodal/distant metastasis. CT can be particularly useful for detection of lymph node involvement, while MRI may be helpful in distinguishing from benign (non-cancerous) disease. The presence of jaundice with GBC is associated with poor prognosis. For cholangiocarcinoma (CCA), the optimal diagnostic approach is core needle biopsy.8
References
- Fusco N, Bosari S. HER2 aberrations and heterogeneity in cancers of the digestive system: Implications for pathologists and gastroenterologists. World J Gastroenterol. 2016;22:7926-7937. doi:10.3748/wjg.v22.i35.7926
- NCCN Guidelines for Patients®. Esophageal Cancer (2024). https://www.nccn.org/patients/guidelines/content/PDF/esophageal-patient.pdf
- Bartley AN, Washington MK, Ventura CB, et al. HER2 testing and clinical decision making in gastroesophageal adenocarcinoma; Guideline from the College of American Pathologists, American Society for Clinical Pathology, and American Society of Clinical Oncology. Arch Pathol Lab Med. 2016;140:1345-1363. doi:10.5858/arpa.2016-0331-CP
- Petrillo A, Smyth EC, van Laarhoven HWM. Emerging targets in gastroesophageal adenocarcinoma: What the future looks like. Ther Adv Med Oncol. 2023;15:17588359231173177. doi:10.1177/17588359231173177
- Esophageal Cancer – Medical illustrations. https://www.cancer.net/cancer-types/esophageal-cancer/medical-illustrations
- Johns Hopkins Medicine Pathology. Gallbladder and Bile Duct Cancer. Anatomy and Physiology. https://pathology.jhu.edu/gbbd/anatomy-physiology
- NCCN Guidelines for Patients®. Gallbladder and bile duct cancers (2023). https://www.nccn.org/patients/guidelines/content/PDF/gallandbile-hp-patient.pdf
- National Comprehensive Cancer Network®. NCCN Clinical Practice Guidelines in Oncology. Biliary Tract Cancers (Version 1.2025) https://www.nccn.org/professionals/physician_gls/pdf/btc.pdf
All URLs accessed April 12, 2025